
Is Toothmousse all it’s cracked up to be for Hypomineralisation?
We see several hundred of patients a year with hypomineralisation. We would say more than three-quarters of them walk in having been told to use a CPP-ACP product, predominately Toothmousse. However, it is not cheap and is an extra step every night to do. Like all things in dentistry, we need to ask, what is the actual benefit of this?
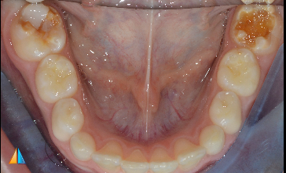
Severe hypomin with PEB: 6/46
Will Toothmousse do much here?
The Hype
Tooth Mousse (CPP-ACP) is widely recommended for children with molar incisor hypomineralisation (MIH), at least in Australia and New Zealand.
The rationale behind tooth mousse is really quite appealing and seems to make some sense
· It increases bioavailable calcium and phosphate
· It supports remineralisation and reduces demineralisation
· It may reduce sensitivity
But the key question remains:
Does this actually translate into meaningful clinical improvement in hypomineralised teeth?
Remineralisation
In lab based studies, CPP-ACP can increase mineral content in enamel. However, hypomin lesions are deep structural defects. They usually are the full-thickness of enamel deep. Can CPP-ACP penetrate this far? No, it works on the surface. Clinical studies show modest or inconsistent improvements and no clear superiority over fluoride…
Sensitivity
There is some evidence CPP-ACP may reduce hypersensitivity over time, but results are variable and not clearly superior to alternatives. It may help mild cases but is not reliable for moderate–to-severe sensitivity. Silver Diamine Fluoride (SDF) is registered in most countries as a desensitising agent and not for caries treatment. It is quite an effective desensitisation treatment for sensitive teeth and involves one, or two applications, not applying a paste every night for monhts on end. We do have a free online course about SDF, with a small component about hypominerlisation. PREVENTIVE APPROACHES TO DENTAL CARIES - A REVIEW OF MINIMALLY INVASIVE DENTISTRY — Kids Dental Tips. In our hands it is the most effective treatment for hypomin related sensitivity.

Post SDF treatment, unfortunately, it does stain it a bit black…
Prevention of breakdown
There is little high-quality evidence that CPP-ACP prevents post-eruptive breakdown in MIH molars. It does not address the underlying structural weakness. Essentially, if a tooth is going to break, it will break whether you put tooth mousse on or not.

PEB on #16
Anterior Hypomineralisation?
Anterior hypomineralisation is more of an aesthetic concern for patients than a functional one. These teeth do not tend to breakdown as badly as they don’t suffer as much of an occlusal load. But they can look a bit ordinary.
There a host of options you can use to try to manage these conservatively. The worst thing you can do is pick a drill up! We have another post about these techniques: Anterior Hypomineralisation - How To Improve The Aesthetics — Kids Dental Tips
But briefly, we use toothmousse for microabrasion treatments where we seem to get a reasonable outcome in yellow/brown lesions

Management of anterior lesions with a combination technique. We used Toothmousse as part of microabrasion
Clinical Applications for Tooth Mousse - Evidenced bases (and anecdotal)
Ok, so looking through the evidence and summarising above
It won’t prevent breakdown
It won’t materially remineralise or change the hypomineralised lesions. It is no better than fluoride and possibly less effective
It may reduce sensitivity in mild cases if used consistently over a reasonable period of time
But does this have a meaningful impact on patients and should they be sold this product? Short answer, despite what your lecturers may have told you, is no!
Conclusion
If the patients are using a 1450ppm toothpase, twice per day, flossing and are regular attenders of the dentist that is generally a more cost-effective approach. Management of breakdown will depend on the tooth itself and the patient. To reduce sensitivity, we generally apply SDF to the lesions prior to any treatment, including sealants.
So out of the several hundred patients a year we see with hypomin, how many in our practice get recommended Toothmousse - it would be the handful of patients having microabrasion treatment. We don’t even stock it at our clinic - we send them to the local pharmacy or supermarket.
References (if you want to see some evidence)
https://pubmed.ncbi.nlm.nih.gov/39685613/
https://www.mdpi.com/2304-6767/11/3/80
https://pmc.ncbi.nlm.nih.gov/articles/PMC11865127/
https://www.sciencedirect.com/science/article/abs/pii/S0300571216301889
https://pmc.ncbi.nlm.nih.gov/articles/PMC9775541/
https://www.nature.com/articles/sj.bdj.2018.814