
Orthodontic Considerations in the Paediatric Population - Part 2
This is part 2 of the orthodontic series. We had some common questions submitted to us to discuss with Dr Caitlin Giulieri.
Part 1 is at: Orthodontic Considerations in the Paediatric Population - Part 1 — Kids Dental Tips
Q: What tips do you have for the general dentist with regards to referring a child for orthodontics?
A: If the general practitioner has any doubt whether or not a child is ready for an orthodontic consult, then it is probably best to send them. This is better than missing the boat for ideal timing of interventions, and allows the family and orthodontist to develop rapport and work towards a common goal - whenever that may be indicated.
If the child is anxious and the GDP is concerned that they wouldn’t cope with orthodontics, it is still good to send them for a consultation. Orthodontists work extensively with children; there are few children where anxiety is a significant barrier for good orthodontic care. In fact, often an early meet and greet allows the child to become familiar and develop rapport with the orthodontist who will be treating them in the future.
Please palpate for the canines at age 9/10 in the buccal sulcus and follow up with appropriate imaging (an OPG) or a referral to an orthodontist if they are not palpable. The earlier impacted canines are diagnosed, the more treatment options are available. Don’t wait until age 12 as there may be reduced options by then!

Early referral and management is crucial for severely hypomineralised first permanent molars – again, a late referral may result in reduced treatment options.
Typically, there is not much an orthodontist can do when the child is in full primary dentition. They should usually have their 6’s and upper 2-2 before seeing the orthodontist. Unless they have impacted incisors or impacted 6’s, in which case early interventions are indicated.
Q: Is a Lower Lingual Arch (LLA) space maintainer required when there is premature loss of the lower c’s?
A: An LLA would be appropriate for the bilateral early loss of lower E’s, however, I don’t usually recommend them for early loss of the canine’s. Space closure after early loss of the canine’s usually arises from the incisors shuffling back to gain more space, NOT from posteriors moving forwards. In fact, unnecessary LLA’s can increase the risk of the 7’s impacting as the 6’s have not moved forwards into the leeway space as designed.
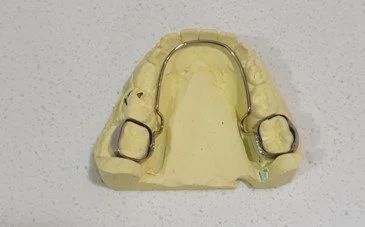
LLA on a model

Impacted 7’s with LLA present
If one lower canine is lost early (due to caries or trauma), then often it is a good idea to extract the other lower canine, as unilateral loss can result in a midline shift of the permanent incisors (unless the midline shift has already occurred). Also, lower canine’s can be lost early due to inherent incisor crowding as the root of the canine is resorbed with the eruption of the incisors. In these cases, the space is going to be lost BECAUSE of the existing crowding. They will not become crowded because of the early loss of the canine.
Instead, it is better to balance the early loss by extracting the other lower canine, let the incisor crowding improve itself and monitor for when the lower canines are due to erupt. By this stage you can get a better assessment of the crowding and there’s time for more growth to reduce the severity of the crowding (transverse inter-canine width, leeway space and antero-posterior jaw length growth). The lower canines rarely impact but often erupt rotated or buccally crowded, which can be corrected orthodontically in the permanent dentition when the rest of the crowding is ready to be resolved. Even if they stay unerupted, space can be opened or created so long as they remain in a good buccal position.

Poor oral hygiene around an LLA
It's important to weigh up that a LLA is a lot of bulk to keep clean, and it needs to stay in for many years which can burn out a kid if placed really young. They can debond somewhat frequently and can be a pain for all involved!
We have one more series of posts to go!